Tender Tracking Software for MedTech Bid Teams
Answer first: Tender tracking software for MedTech and pharma manufacturers is a bid-desk system: multi-country sources, catalog-aware fit scores, deadline owners, no-bid audit, and a clean handoff into tender response automation. It is not hospital purchasing software and not a CRM that only pings “new RFP.” Orbid AI (formerly MedStrato) covers opportunity feed plus a native response agent so chase and file stay connected.
Book a demo · orbid.dev · shortlist context in the 2026 best-of.
Tracking vs response (do not collapse them)
Tracking finds and prioritizes opportunities. Response automation fills the technical pack. Mature desks need both. Many teams start with a spreadsheet tracker, win the chase, and still lose on missing CE files at submission. Pair tracking with the 5-step agent loop.
Capability scorecard (manufacturer lens)
| Capability | Spreadsheet tracker | Generic CRM alerts | MedTech bid-desk tracker |
|---|---|---|---|
| Multi-country portals (TED, national, GPO) | Manual paste | Partial | Native or curated feeds |
| Catalog-overlap / fit score | No | Keyword only | SKU / regime aware |
| Certificate validity on “go” | No | No | Yes / RA gate |
| Owner + stage pipeline | Fragile | Sales stages | Bid-desk stages |
| Handoff to response agent | Link dump | Evidence pack ready | |
| No-bid audit log | Optional notes | Rare | Required |
Where spreadsheets break
Shared Excel trackers do not know that your SKU lost CE validity last Tuesday. They also do not stop two regional teams from double-chasing the same lot—a capacity tax that looks like “more pipeline” and feels like burnout. Past roughly twenty live opportunities, Excel becomes a risk system, not a tracker.
- No single owner when deadlines slip
- No structured no-bid reason for learning
- No link from opportunity to catalog readiness
- No export path into the buyer’s template
What “catalog-aware fit” means
Keyword alerts fire on “ultrasound” while your sellable SKU is expired in one regime and ready in another. A manufacturer tracker should score fit against your catalog and certificate state—not generic industry news. That is the same state model a technical-pack response agent uses when it matches lines.
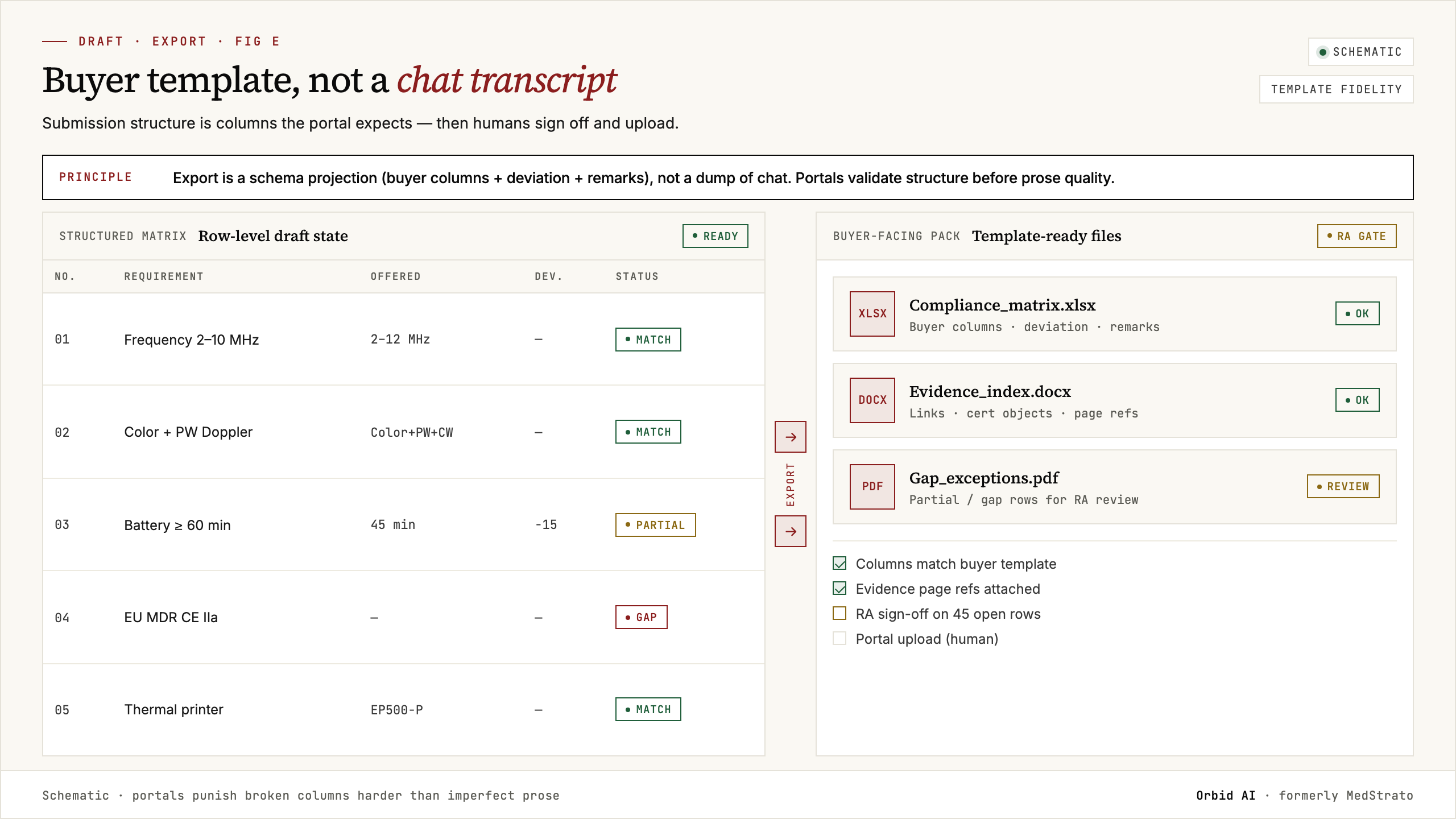
Tracking → response handoff
The expensive failure mode is winning the chase and losing the file. On “go,” the desk needs:
- Lot and deadline locked with an owner
- Pack intake path (XLSX / PDF / ZIP) without retyping the opportunity
- Partial-match policy ready for humans
- RA visibility on certificate gaps before pricing politics
Orbid AI is built so opportunity context and response execution stay in one manufacturer workflow—not a separate “intel SaaS” and a disconnected agent.
How this differs from Cube-class intel and TenderEyes collab
- Life-sciences intel suites excel at market visibility and sometimes pricing simulation; they are not always the best line-level device matrix tools.
- Bid collaboration platforms excel at Microsoft 365 content and approvals; trackers still need catalog/regime awareness.
- Horizontal RFP libraries do not track device tenders as structured state.
Full field map: tender management software comparison.
Buying criteria for 2026
- Is the product built for regulated device catalogs—not only generic B2B RFPs?
- Can RA block a “go” without email archaeology?
- Does “go” hand off into match/comply/export, not only a folder link?
- Multi-country sources without forcing a second spreadsheet?
- SOC 2 / data residency suitable for enterprise tenders?
KPIs for tracking desks
- Time from notice to owner assignment
- % opportunities with catalog fit scored before go/no-go
- Duplicate chase rate across regions
- Go decisions that reach sealed export on time
- No-bid reasons coded for learning
Compare tools in our software comparison and 2026 best-of, review features, then book a demo or open orbid.dev. Research shell: State of MedTech Tender Response 2026.