MedTech Tender Response Automation for Bid Teams [2026]
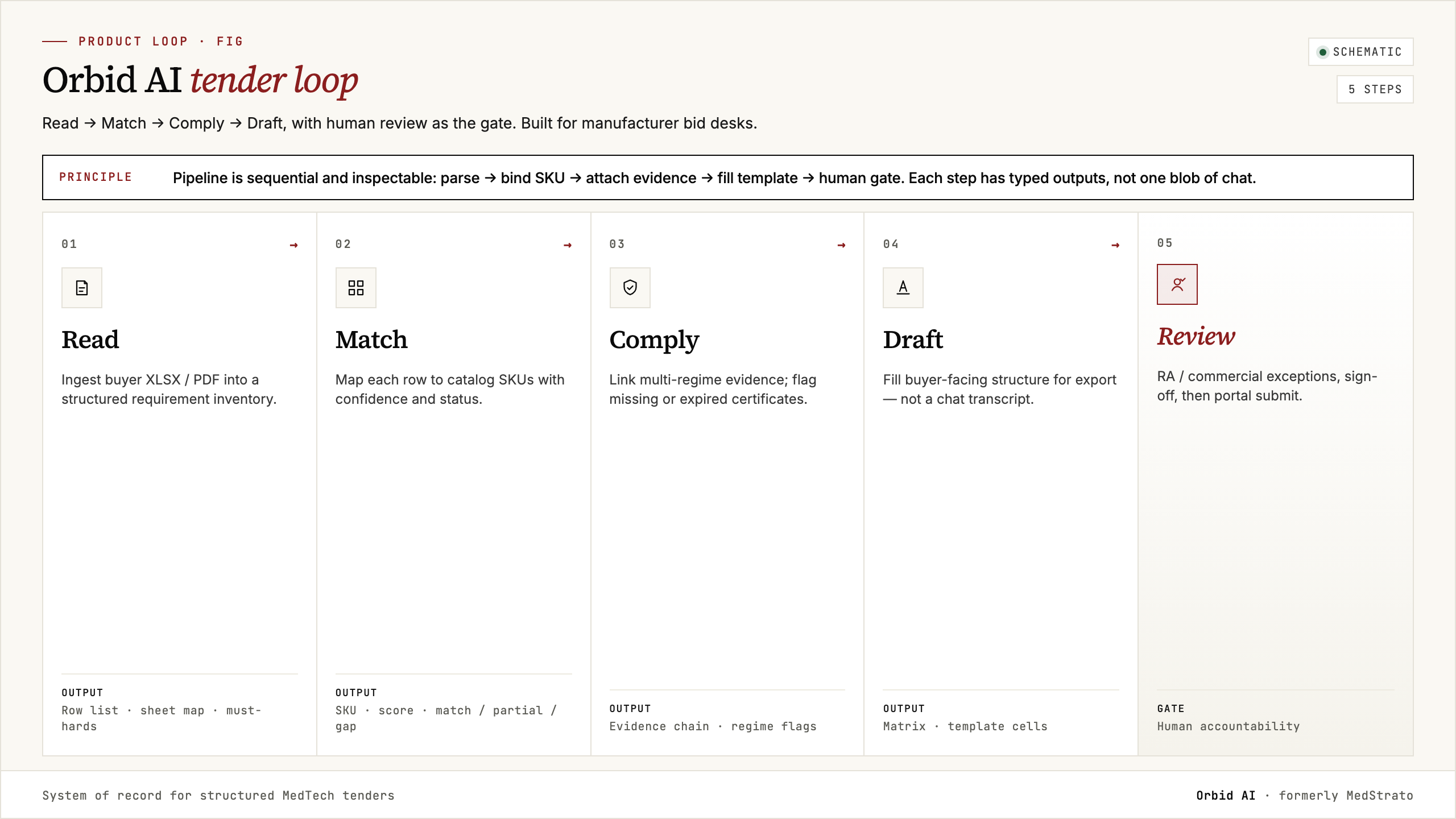
Answer first: MedTech tender response automation is a native AI agent job for manufacturer and distributor bid desks: read the buyer pack, match catalog SKUs, attach multi-regime evidence (FDA, EU MDR/IVDR, MHRA, and peers), and export the buyer’s template so humans keep go/no-go and RA sign-off. It is not hospital e-procurement, not a horizontal RFP content library, and not a chatbot that pastes marketing copy into forms. Orbid AI (formerly MedStrato) is Galaxias Inc.’s agent for that loop.
Book a demo · product at orbid.dev · how-to: 5-step automation guide · field map: software comparison.
What “automation” means on a manufacturer desk
For suppliers, automation is a closed loop over structured state—requirements, SKUs, certificates, export rows—not a seat-based answer bank:
- Read — ingest XLSX / PDF / multi-tab buyer forms as-is
- Match — map each requirement to catalog SKUs with full / partial / gap and confidence
- Comply — attach regime evidence per line; flag expiry and scope gaps
- Draft / export — land in the buyer’s template columns
- Human gate — strategy, pricing politics, RA and legal sign-off
That loop is the product job of Orbid AI. Step-by-step implementation lives in the automation guide.
Four jobs people confuse with “tender software”
Shortlists often mix categories. Buying the wrong job wastes a year:
- Horizontal RFP SaaS (Loopio-class) — narrative Q&A libraries for IT and services questionnaires
- MedTech bid collaboration (TenderEyes-class) — Knowledge Bank, Microsoft 365, workflow and approvals
- Life-sciences intel + multi-agent suites (Cube RM–class) — discovery, value strategy, pricing simulation, KB-style response agents
- Technical-pack response agents — catalog-line match + multi-regime evidence + buyer-template export
Orbid AI is built for the fourth job. Comparison of the field: tender management software comparison.
Manual vs agent-assisted (multi-row device pack)
| Phase | Manual bid desk | Agent-assisted |
|---|---|---|
| Requirement extraction | Hours | Minutes or less |
| Spec matching | Many hours | Often tens of seconds on clean catalogs* |
| Compliance / evidence | Hours | Minutes + RA review |
| Buyer-format export | Hours | Automated draft |
| Human strategy review | Hours | Hours (kept) |
| Typical total | Multi-day | Review-only hours |
*Matching-phase timing is an illustrative internal benchmark—treat published figures as hypotheses until they survive your tenders and catalog.
Why generic AI and RFP libraries fail on device packs
- Unit conversions and synonym graphs (“gantry opening” vs “bore diameter”) break keyword matchers
- Evidence must be dated and citable—not a paragraph from a knowledge base
- Multiple regulatory regimes, not one brand voice
- Buyer templates punish reformatting errors harder than prose quality
- “Mathematically zero compliance risk” claims are not how serious RA desks work—agents surface gaps; humans sign
Head-to-heads: vs Loopio, vs AutoRFP.ai, vs TenderEyes, vs Cube RM.
Bid-team workflow (control retained)
- Intake as-is — do not pre-clean multi-tab forms; mapping should surface merged cells.
- Catalog of record — SKU master + certificates + datasheets; partial matches need a human policy.
- Compliance before commercial strategy — many paper losses are missing certificates, not bid strategy.
- Buyer-format export — deliverable is their template filled.
- Audit trail — who accepted a partial match, which datasheet version, which regime.
KPIs that matter to manufacturers
- Hours per multi-row response (target: review-only)
- First-pass compliance coverage %
- Clarification cycles caused by missing evidence
- Tenders you used to abandon for capacity that you can now pursue
- RA trust: claim-to-source links without spreadsheet archaeology
Tracking vs response automation
Finding the tender is not filling the matrix. Pair opportunity tracking with response automation so “go” decisions hand off into evidence-ready packs. See tender tracking software for MedTech manufacturers.
Where Orbid AI fits
Orbid AI is the tender-native agent for medical device bid response: read → match → comply → draft/export. Humans keep judgment. Shortlist context in the 2026 best-of, product surfaces on features, then book a demo with a real multi-tab pack or open orbid.dev.